 read pdf version
read pdf version
Protecting the entitlement of elderly people in care to the
same rights,
freedoms, privileges and necessities of life as other citizens
Families Allied to Influence
Responsible Eldercare
Presentation to the
Standing Policy Committee on Health and Community Living
June 17, 2003
by
Families Allied to Influence Responsible Eldercare (FAIRE)
Box 969 Cochrane, Alberta, T4C 1B1
Tel: (403) 932-5557
Email: bevmckay@telus.net
Presenters:
Bev McKay, Founder/President
Stan Henderson, Family Member
Table of Contents
Introduction .........................................................................................1
Background ........................................... .............................................2
Proposals ............................................................................................3
a) Legislative Standards
b) Inspections/Enforcement
c) Funding
d) Canadian Criminal Code
e) Vulnerable Adults Protection Commission
Conclusion ..........................................................................................6
Summary of Anecdotes Recorded in FAIRE's Confidential Database ...............7
A Portrayal of Abuse, Neglect and Poor Care of Vulnerable Seniors ...............8
In Alberta's Nursing Homes
Personal Testimonies of Families ............................................................13
Appendices ........................................................................................35
- Appendix A: FAIRE's efforts to advise the Alberta government
of residents' experiences of abuse, neglect and poor care,
and the urgent need to address the root causes.
- Appendix B: Current Minimum Staffing Standards in Alberta
- Appendix C: Recommended Staffing Standards to Accommodate
Residents Increased Needs and Levels of Acuity
- Appendix D: What's An Autonomous Family Council?
Introduction
Families Allied to Influence Responsible Eldercare (FAIRE) was founded in 1998 by a small
group of families in response to their loved ones' experiences of abuse, neglect and poor care in
an Alberta nursing home and to their own feelings of helplessness and fear to speak out. It is in
this context that FAIRE formalized to educate and support families and to work alongside them
to protect their loved ones' fundamental rights and improve their quality of life and care.
FAIRE is very honoured to be recognized provincially and nationally for its contributions to the
work being done across the country to raise public and government awareness to the
mistreatment of frail older persons in publicly-funded care facilities and to press for a plan of
government action to combat elder abuse in these settings. Examples of FAIRE's work include:
· November 2002: FAIRE was selected to give a presentation on institutional abuse and
neglect of older persons at the Ontario Elder Abuse Conference co-sponsored by the
Ontario Network For the Prevention of Elder Abuse and the Ontario Seniors' Secretariat.
· May 2002: Sponsored a public forum to launch our researched-based report, The
Shame of Canada's Nursing Homes, which was distributed nationally. The report
examines nursing home abuse and neglect from a national perspective. Our guest
speaker was lawyer/researcher Charmaine Spencer, Gerontology Research Centre,
Simon Fraser University. More than 125 people attended the event.
· March 2002: Launched our educational/informational website which was made possible
by a donation from the South Calgary Rotary Club.
· 2002 and 2003: Received grants from Imperial Oil's Volunteer Involvement Program for
the maintenance of our website which is being used as a resource by families, students,
researchers, health care professionals and seniors' organizations
· 2001-2003: Gave presentations to seniors' organizations, inter-agency homecare
workers, CARP Calgary Chapter, the Calgary Kiwanis Club, Kerby Centre and L'Arche
staff, students enrolled in the University of Calgary Vulnerable Adults Education Program
and the Victorian Order of Nurses Personal Careaide Program
· March 2001: Made a submission to the Romanow Commission
· 2000 2003: Gave media interviews to CBC Radio and Television, QR77, CKNW,
A Channel, Calgary Herald, Edmonton Journal, Cochrane Times, Cochrane Eagle,
Western Producer and Reader's Digest
· September 2000: Sponsored a public forum featuring Dr. Kenneth Rockwood, Professor
of Geriatric Medicine, Dalhousie University
· March 2000: Co-sponsored a community consultation on the Protection for Persons In
Care
Act
· July 1999: Hosted guest speaker, Michael Kendrick who is known internationally for his
advocacy and lectures and work in the areas of mental health, disability and ageing.
· June 1999: Initiated an analysis by the University of Calgary of the Health Facilities
Review Committee routine investigation reports; conducted our own review of the
inspection rate of Alberta's nursing homes
· From 1999: Continue to advise the Alberta government, its Ministers and MLAs of the
issues facing seniors in care and the pressing need for remedial action (See Appendix
A).
1
Background
Since late 1999, FAIRE has documented 189 anecdotal experiences of elderly residents,
reported to us by concerned families and, increasingly, by concerned health care professionals.
More than seventy-three percent (73%) of these anecdotes involve residents who suffered harm
or were placed at risk of serious injury. Over nine percent (9%) relate to possible preventable
deaths. Additionally, approximately 3000 abuse allegations have been reported under Alberta's
Protection For Persons In Care Act. Of the 542 allegations reported in the Act's 2001/2002
fiscal year alone, more than fifty-seven percent (57%) potentially held some criminal law
elements (Spencer C. 2002). While these numbers are alarming in themselves, research
indicates incidents of abuse, neglect and crimes committed against nursing home residents are
grossly under-reported.
In 2001, FAIRE conducted an extensive literature review to examine institutional abuse and
neglect of older persons from a national perspective and the many factors that facilitate and
permit this unconscionable social problem in our health care system. Our findings, published in
a report called The Shame of Canada's Nursing Homes, suggest abuse and neglect is a
widespread regular aspect of institutional life. They also show research is lagging in this area
and provincial governments are slow even reluctant - to acknowledge the existence of the
problem and their part in creating it. For years, short-sighted government policies regarding our
nursing homes have resulted in chronic underfunding, under-regulation, lax inspections, lax
enforcement of standards and the lack of sanctions against facilities that cause residents harm
or place them at serious risk. The report concludes that without the political will to effect
change, the situation in our nursing homes will likely worsen.
Recent media reports on mistreatment and wrongful deaths of the elderly in nursing homes in
Alberta and other provinces are awakening the general public to the realization that our nursing
homes are not the safe havens they believed them to be. Indeed, people are now learning that
our long-term care system is so seriously flawed and under-resourced that even the basic care
requirements of many residents are not being met. As a result, more and more families are
hiring private caregivers to help feed, dress, toilet, bathe, groom, change incontinent wear, walk
and give mouth care to their loved ones. For those families who cannot afford to hire help,
many are providing the care themselves, often on a daily basis and at considerable cost to their
physical and emotional well-being. What the media are truly revealing to the general population
is that provincial governments have no comprehensive strategy for dealing with the long-term
care needs and vulnerability of nursing home citizens and our aging population or the criminal
acts perpetrated against them. This oversight is significant considering there is an estimated
one-quarter million seniors living in care institutions in this country and that Canada's population
of people over 65 is expected to reach 5 million in less than a decade.
2
Proposals
We offer the following 5 proposals which we hope this Standing Policy Committee will consider
and support. The first three proposals relate to Alberta Health & Wellness and the last two to
Alberta Justice.
Legislative Standards
1) FAIRE proposes that the Alberta government take immediate steps to reform the
Nursing Homes Act and Regulations so as to set out precise comprehensive standards.
Specifically, we call for standards that: relate directly to residents' individual care needs
and levels of acuity include a Residents' Bill of Rights specify the responsibilities
of direct-care staff and the nursing and personal care services and supports to be provided
set out best care practices specify minimum staff-to-resident ratios and the
mandated training/education levels for nurses and aides ( See Appendix C) require
each nursing home to have a nurse practitioner on staff to provide assessment of and direct
care to residents specify strict parameters around the use of chemical and physical
restraints require facilities to develop abuse protocols, procedures and guiding
principles and to routinely assess for, and address risk factors that contribute to the
occurrence of abuse require nursing home owners/operators to give a resident and/or
his or her substitute decision-maker, upon request, access to the resident's personal record,
meaning all recorded information relating to that resident, for the purpose of reviewing the
record or copying it at the person's expense require each facility to support the
establishment of an Autonomous Family Council (See Appendix D)
Increasingly, families are reporting abuse, neglect and poor care of their loved ones, as well as
marked differences in the level and quality of care from one facility to another and from one shift
to another within the same facility. We believe these conditions are directly associated with the
scant and vague standards set in Alberta's Nursing Homes Act and Regulations which have
remained virtually unchanged for more than 17 years. These outdated pieces of legislation are
failing to address the complex needs and illnesses of people currently in care - 68% of whom
assess as requiring a high level of service and care (Alberta Health & Wellness Resident
Classification 2001/2002). The impact of deficient standards in this province is clearly conveyed
in the disturbing personal testimonies and photographs in this submission.
Inspections/Enforcement
2) We propose that the Alberta government dissolve the Health Facilities Review
Committee and replace it with a body of independent, highly trained and qualified
inspectors, including nurse practitioners, mandated to: conduct annual inspections
of every nursing home based on standards set out in the reformed Nursing Homes Act and
Regulations monitor for and enforce compliance of standards cite violations and
take strong and swift enforcement action against nursing homes that violate health and
safety standards or that cause residents harm or place them at risk of serious injury or
death
Alberta's Health Facilities Review Committee, established in 1973, consists of two Members of
the Alberta Legislative Assembly and ten citizens. It is not a requirement that members of the
3
HFRC have professional health credentials (Minister of Health & Wellness correspondence to
FAIRE). The mandate of the Committee is to monitor and investigate the quality of care,
treatment and standards of accommodation provided to patients and residents in health care
facilities throughout Alberta (1998 Committee brochure). Astonishingly, however, the
Committee is not mandated to investigate whether a facility is in contravention of the standards
set out in the Nursing Homes Act and Regulations, nor is it mandated to enforce the standards
or impose sanctions in relation to these pieces of legislation and, it cannot address general
nursing practice issues as they pertain to the professional conduct or competency of nurses
(Committee correspondence to FAIRE). This information from the Committee allows us to see
that the health, safety and well-being of nursing home residents in this province are not, and
have never been monitored or investigated to legislative standards or best care practices. At
the same time, it allows us to understand why residents in this province are so vulnerable to
neglect and poor care --- why no resident care issues are reported in Committee routine
investigation reports, and --- why no sanctions have ever been levied against nursing homes for
violating regulatory standards or jeopardizing residents' health, safety and very lives. While
well-intentioned, we believe this Committee, "constituted to provide the Minister and Albertans
with an ordinary citizen's perspective of the quality of care being provide" (Minister of Health &
Wellness correspondence to FAIRE) is inadequate to the task of identifying, assessing and
investigating the many issues impacting residents quality of care and quality of life.
Funding
3) We propose that the Alberta government provide funding that meets the individual
needs and levels of acuity of citizens in Alberta's nursing homes, and that additional
funding go directly toward higher wages and increased benefits for direct-care staff.
Chronic underfunding of Alberta's nursing homes seriously undermines the ability of
owners/operators to deliver the level of care and protection that residents desperately need and
so rightfully deserve. It also speaks to government policy that fails to recognize the relationship
between low dollar allocations to the nursing home sector and the far-reaching negative effects,
including:
a) The deterioration of residents' health, functioning and quality of life due to inadequate or
non-existent rehabilitative/therapeutic/medical services and supports;
b) Low staff-to-resident ratios which result in heavy workloads, staff burnout and low staff
morale which contribute to poor care and increase the potential for abuse and neglect;
c) The hiring of untrained unskilled personal care staff which is a key factor in resident injury
and neglect which, in turn, results in costly hospital admissions;
d) Low staff wages which result in high staff turnover, an inadequate pool of available skilled
staff, and the indiscriminate hiring of people who are inappropriate for this field of work.
Alberta's 2001/2002 expenditures for facility-based continuing care services totaled
approximately $575 million (Health Authorities Audited Financial Statement) --- an increase of
about $120 million since 1996/1997. Despite these increased funds, the critical staffing issues
noted above remain unaddressed.
4
Canadian Criminal Code
4. We propose that Alberta Justice be diligent in enforcing the following sections of
the Canada Criminal Code (Part VIII) with respect to crimes committed against
citizens living in nursing homes and other care settings in Alberta.
·
Duty of persons to provide the necessaries of life: S 215 (1)(c)(i)(ii); 215(2)
·
Duty of persons undertaking acts dangerous to life: S 216
·
Duty of persons undertaking acts: S 217
·
Criminal negligence: S 219
·
Causing death by criminal negligence: S 220
·
Causing bodily harm by criminal negligence: S 221
·
Homicide: S 222
·
Death that might have been prevented: S 224
·
Death from treatment of injury: S 225
In 1986, Criminologist Birthe Jorgensen published a research paper, Crimes Against the Elderly
In Institutional Care. The paper is based on Dr. Jorgensen's analysis of complaints about
treatment of residents in nursing care facilities brought to the attention of Concerned Friends of
Ontario Citizens in Care Facilities. Her findings revealed that approximately 46 percent of 56
detailed complaints received held sufficient grounds for the laying of criminal charges of theft,
assault or breach of the legal duty to provide the necessaries of life or proper medical care
established by certain sections of the Canadian Criminal Code. Although Dr. Jorgensen
acknowledged there are obstacles to criminal prosecutions, including the vulnerability of elderly
victims to retaliation and the unfamiliarity of much of the general public, including the police and
crown prosecutors, she nevertheless concludes that such prosecutions can and should be
initiated. FAIRE strongly supports this view.
Vulnerable Adults Protection Commission
5. FAIRE proposes that the Alberta government dissolve the Protection for Persons in
Care Act and create an Act that establishes a Vulnerable Adults Protection
Commission to operate as an independent agency under Alberta Justice. This
Commission would comprise experts in the fields of medicine, gerontology, criminology, law
enforcement, rehabilitation, mental health and forensic pathology mandated to identify and
investigate incidents of abuse, neglect and wrongful deaths of vulnerable adults in publicly-
funded care settings in Alberta with the aim of affording victims protection, treatment,
continuity of care and equal access to the criminal justice system. The commission would
also routinely assess for, and address systemic factors that may contribute or lead to abuse,
neglect and wrongful deaths.
Alberta's Protection for Persons In Care Act, enforced in 1998, is currently undergoing a five
year review. This law, while well-intentioned, has been strongly criticized in the community on
several different grounds, including its failure to ensure alleged victims protection and access to
the criminal justice system. Indeed, as government statistics show, only 5.1% of the 542 cases
in 2001/2002 were referred to the police yet, as previously stated, over 57% potentially held
some criminal law elements (Spencer C.) Spencer explains that while, "the specific actions in
5
the cases might not reach the level of criminal intent, or serious harm to warrant a criminal
charge ... often those determinations are being made by consultants doing the investigation,
not the police." Furthermore, government policy in this province allows Regional Health
Authorities to make similar determinations based on their own investigations of potential crimes
in care facilities (e.g. March 2002 Calgary Health Region investigation into the alleged sexual
abuse of an 88-year-old stroke patient of a Calgary hospital; December 2002 Capital Health
Authority investigation into the preventable death of a paralyzed 72-year-old respirator-
dependent resident of an Edmonton nursing home). The victimizations of the sort described in
these two cases and in the majority of PPIC allegations are similar to those examined in Dr.
Jorgensen's 1986 report mentioned above. In the final analysis, Jorgensen concludes,
"Criminal prosecutions probably will be more likely to effect positive changes in conditions in
nursing homes than the current enforcement mechanisms of the Ministry of Health." Today, a
growing number of prosecutors, coroners, medical examiners and law enforcement officers in
the United States are expressing this same view and are working collaboratively to pursue some
form of justice for nursing home victims (Special Report 2002: St. Louis Post-Dispatch).
Conclusion
FAIRE views this submission as important for several reasons. First, it provides an opportunity
for concerned families to be heard at the government level, and for this government to learn
what nursing home life is like for increasing numbers of our most vulnerable citizens in care.
Secondly, it speaks to the need for government and policy makers to involve knowledgeable
families and other informed stakeholders in policy-decisions that affect the lives of long-term
care residents. Moreover, it enables our elected officials and the general public to realize that
nursing home citizens in this province have been left seriously vulnerable by deficient
regulation, inspection, investigation and funding. At the same time, it offers solutions for
bringing about changes that would make a difference in the lives of people who live and work in
care facilities. Finally, it calls for a political response that commits to ensuring nursing home
residents the best possible quality of care and quality of life.
We believe our proposals are consistent with the vision of this government providing effective
protection and quality care to our frail elderly while honouring their right to a secure environment
and equal access to the criminal justice system. We look forward to the opportunity to work
collaboratively with government and to be part of an expert advisory committee which we
suggest be established to address this pressing issue.
6
Summary of Anecdotes
Recorded in FAIRE's Confidential Database
General Concerns: 32
Possible Preventable
Deaths: 18
Injury: 94
At Risk: 45
Total Anecdotes Recorded: 189
Examples of residents'
Examples of residents being placed
experiences that resulted in
Examples of premature deaths
at risk of injury, illness, abuse or
injury, illness, trauma and health
death
decline
· A paralyzed respirator-
dependent resident died when
· Units are left unsupervised; call
· Physical and sexual assault
staff failed to respond to alarm
bells for assistance go unanswered;
monitors indicating the respirator
staff are unaware of fire drill
· Life-threatening pressure sores
had failed
associated with infrequent or
procedures
· A resident wandered unnoticed
no repositioning
· Residents are left in their waste for
out of the nursing home and was
· Undetected/untreated urinary
hours at a time
later found dead in a nearby
tract infection, pain, fractures,
· Colostomies rupture and catheter
field.
pneumonia, sepsis,
tubes plug due to inadequate
malnutrition and dehydration
· A resident died of asphyxiation
monitoring
after becoming trapped between
· Life-threatening bowel
· Residents are not given adequate
her mattress and a support pole.
obstruction caused by fecal
assistance or time to finish their
· A resident died after being
impaction associated with
meals; meals are taken away
inadequate fluid and poor
dropped from a mechanical lift.
untouched
nutrition
· A resident died after being
· Residents suffer weight loss and
· Drug-induced toxicity, falls
hurled out of her wheelchair
health decline due to inadequate food
causing fractures and bruising,
when it rolled down an indoor
intake, undetected swallowing
neurological disorders,
ramp and impacted a wall.
difficulties or medical condition
swallowing difficulties, coma
· A resident fell, his head hitting
and loss of functioning
· Residents suffer adverse drug
the floor. Two unassessed falls
reactions due to being administered
· Muscle contraction and atrophy
followed. The resident
wrong or multiple medications; nurses
attributed to the use of physical
subsequently died.
dispense medication but do not
restraints and/or inadequate or
ensure residents take it; medication
· A resident died after failing to
no exercise or physiotherapy
carts are left unlocked
receive treatment for a
· Mouth thrush, gum disease and
and unsupervised
gangrenous foot.
full-tooth extraction caused by
· Residents are hospitalized in diabetic
· Two residents died after failing to
inadequate or no mouth care
coma caused by inadequate
receive treatment for 1) a
· Unskilled/inappropriate handling
monitoring of blood sugar levels
reported gastrointestinal bleed 2)
of mechanical lifts and
reported symptoms of
· Residents wander out of the facility
wheelchairs resulting in
pneumonia.
unnoticed and are found lost and
residents suffering serious
injured in the community
· A resident died from 3rd degree
injury
burns caused when his clothes
· Ambulatory residents are restrained in
caught fire in a smoking
· Residents requiring toileting
wheelchairs or are tied down in
assistance are being put in
incident
their beds
diapers and told to use them
· A resident was left unattended in
and, to their humiliation , they
· Residents' oxygen tanks run empty
the bathroom. He fell to the floor
or are not turned on
do.
and suffered a broken hip. He
· Residents are made to stay in their
died within 10 days of the
beds for hours and even days at a
incident.
time.
7




A Portrayal of Abuse, Neglect and Poor Care of Vulnerable Seniors
In Alberta's Nursing Homes
The following photographs portray some of the tragic nursing home experiences of Alberta's
elderly citizens identified in the previous summary and following testimonies.
The overuse of antipsychotic drugs on this
woman with dementia caused heavy
sedation, resulting in falls that led to these
injuries and a broken hip.
The injuries of this gentleman with dementia
were the result of a beating by his roommate
who suffered the same illness. There was no
staff supervision on the Unit at the time of the
attack.
This gentleman with dementia suffered the
trauma and indignity of being routinely
confined to a wheelchair under a three-way
This woman with dementia suffered
restraint.
prolonged untreated pain due to staff's
failure to detect her obvious symptoms.
8






A Portrayal of Abuse, Neglect and Poor Care of Vulnerable Seniors
In Alberta's Nursing Homes ... continued
This woman's protruding tongue is a
symptom of an irreversible neurological
When the nursing home failed to address this
disorder caused by the overuse of
woman's declining health, the family took her
antipsychotic drugs.
to the hospital. Lab results confirmed
malnourishment, severe dehydration and
pneumonia.
This woman was diagnosed as suffering from
dehydration due to inadequate fluids
When the nursing home failed to treat this woman's
skin condition, the family took her to a specialist
who diagnosed staph infection.
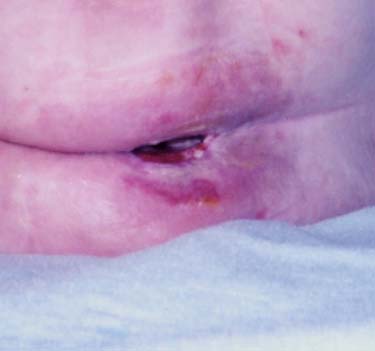
These injuries of unconfirmed cause
While trying to maneuver this man out of a
room, staff inadvertently shut the door on his
were discovered by the family.
9
hand, severing the fingertip.





A Portrayal of Abuse, Neglect and Poor Care of Vulnerable Seniors
In Alberta's Nursing Homes ... continued
A pressure sore open to the spine and
This gentleman's injuries are believed by the
surrounded by dying skin tissue
family to be the result of a physical attack by
his roommate but claimed as self-inflicted by
a government investigator.
The overuse of major tranquilizers caused this
gentleman several falls resulting in a broken
nose and heavy bruising and cuts to his face and
Unskilled handling of a mechanical lift
hands. Staph infection in the cuts went untreated
resulted in this woman falling to the floor,
until the family intervened.
causing a severe head concussion.
Unexplained bruising
10




A Portrayal of Abuse, Neglect and Poor Care of Vulnerable Seniors
In Alberta's Nursing Homes ... continued
This same woman suffered blisters
and bruising on the bottoms of her
feet caused by staff allowing her feet
to drag along the floor as they
pushed her wheelchair rather than
supporting them on the footrests.
The details of the alleged assault of this woman by
her roommate's son and the results of a
government investigation into the incident were
never revealed to her family. However, the family
suspects the heavy bruising on their mother's arm
and the injury to her right toe (opposite) were
inflicted by the alleged abuser.
Unexplained bruising below left eye and
lower lip
Unexplained bruising and broken
skin
11









A Portrayal of Abuse, Neglect and Poor Care of Vulnerable Seniors
In Alberta's Nursing Homes ... continued
In a letter to this woman's son, the facility administrator assures "we will endeavour to
meet the comprehensive needs of (your mo
ther) in a quality and caring fashion." These
words fly in the face of the mother's true experiences as shown below.
Suffering the indignity
of being left exposed
Bad nursing practice
demonstrated by the hazardous
Bug infestation
contaminates her
position of catheter tube
room, bed linens
and fluids
Feces contaminates her
personal space.
Left shamefully exposed with catheter
tube wound beneath her
12
13
A Daughter's Testimony
My father, Frank Gardner, suffered from dementia. He entered a nursing home in
Calgary in January 1997and lived there until his death, in April 1999 at age 74.
My Dad was abused while in care.
Put on the antipsychotic drug Haldol, when he wasn't psychotic. It is a "chemical
restraint". It quickly made him immobile, in a wheelchair, drooling and nonverbal.
Unexplained bruises were observed by us. While sleeping, Dad was beaten up by his
roommate, who also had dementia.
My Dad was neglected while in care.
His hygiene was very poor. One shower per week. Urine soaked. Unsupervised, he
ate soap and had an allergic reaction. Unable to feed himself, he wasn't fed well by
staff, and Mom had to go at least once a day, to feed Dad one good meal. Not
taken to recreational activities, because he wandered. Falls that nobody saw.
Because he was nonverbal, the staff didn't talk to Dad.
Why was my Dad's care in the nursing home so bad? Why were the last years of
his life so miserable? Why was there no respect for his humanity? Why did Dad
work so hard for his country and city, and receive so little when he most needed
care?
Why doesn't our government address this terrible state in our province's nursing
homes, and change things to make them better?
Thank you for listening, but I hope that you will really hear, and then do what is
right.
14
A Wife's Testimony
Recently, while spending time in a waiting room, I picked up a Reader's Digest containing an article on
nursing homes, called Canada's Hidden Crimes. It brought back the horror of my husband's experience of
care and death in an Alberta long-term care facility.
It is five years since my husband died and I continue to feel rage and guilt. Rage at our Health Care System
and guilt that I did not know how to fight effectively for his welfare.
My husband had Alzheimer's but apart from that he was a healthy man. Two weeks after admission to a
Calgary hospital in August of 1996 he could not feed himself, he could not stand or walk. He was secured
in a chair. He engaged in uncontrolled pounding on the tray. The drug was Haldol, administered to keep
him from wandering - a drug banned in the U.S. and, according to drug books not recommended for the
elderly or those with a history of depression. My husband was 83 with life-long depression.
He was transferred to a Continuing Care Centre and taken off the drug. There he experienced gentle
concerned care. They worked hard at helping him to walk and slowly he recovered. Finally he could walk
with me and carry on a conversation. A book of his poetry had been published recently and he was able to
enjoy it with his friends.
Just before Christmas he was transferred to another facility. Initially, I was pleased with the bright
atmosphere so necessary for a person with depression. The staff wanted to know everything about him and
an assessment meeting was held to share the information for effective care. At this meeting my statement
was loud and clear that no change in medication should be made without consultation with me. I
understood there was agreement. What a cruel farce. They paid no attention. There was no continuity of
care. Twelve hour shifts for three days and off for three days and then an assignment elsewhere. For most
of the staff it was just a job. My husband's lifelong apprehension of strangers put him in a fear situation.
When I objected to this parade, the response was, "Oh our patients get used to us all in the course of time."
WE ARE TALKING ABOUT ALZHEIMER PATIENTS HERE! From one day to the next I never knew who
was responsible for his care ... and I was there five days a week.
When he responded in his fear he was termed violent. He did not strike out at me or his friends or relatives
including two young children.
Soon he was walking with tiny steps which I recognized as a forerunner of the Haldol treatment. When I
challenged the staff about his drug situation they denied any change. When I persisted they admitted the
doctor who had prescribed a new drug. My strong impression was that THIS WAS THE WAY IT WAS
GOING TO BE! I was pacified with assurance that it was mild and a low dose. In no time he was once
again in the same state that Haldol had produced.
Now, this recently healthy man looked like a victim of a concentration camp. His skin hung on his bones.
And in this weakened emaciated state he picked up a hospital infection and died. This was accomplished in
the short time between mid-December and the end of February.
I have some questions!
1. What deficiencies within Alberta's health care system are responsible for the persistent use of
potentially dangerous antipsychotic drugs when humane non-pharmacological alternatives are being
practiced elsewhere?
2. In my opinion, failing to withdraw a patient from antipsychotic drugs when he or she presents with
adverse drug reactions and deteriorating health, constitutes abuse and unethical practice. When
treatment proves not in the best interests of the patient, what allows medical professionals to continue
to inflict harm, or worse, to hasten death through bad practice?
3. Medical professionals treated my mentally incompetent husband without my informed consent. More to
the point, they ignored and overrode my decisions regarding his treatment. According to the law, these
practices constitute unlawful behaviour. What allows medical professionals immunity from the law?
15
A Daughter's and Grandson's Testimony
Our frail 85-year-old beloved mother /grandmother entered Alberta's long-term care system at
the age of 85. She suffered severe osteoporosis, violent headaches resulting from two
unsuccessful eye surgeries and short-term memory loss caused by a stroke. At this most
vulnerable and needy time in her life, our loved one found herself caught in a so-called "care"
system that caused her intolerable suffering and harm, robbed her of every dignity, and violated
her fundamental human rights.
In Alberta's long term care system, the mother/grandmother whom we dearly love was...
· Physically assaulted by her roommate's son
· Subjected to multiple psychotropic drugs which took a terrible toll on her health
· Deprived of her ability to walk by being restrained in a wheelchair; she was given no
exercise or physiotherapy
· Put in a small dark room because she called out for help; we often found her there
soaked in urine and sitting in feces; her diapers had no fasteners
· Often left without the use of her dentures, either because they weren't put in or were lost;
during these times she was given a regular diet making it impossible for her to chew her
food; to our knowledge, no assessment was done to determine food
appropriateness or adequacy of food intake
· Bruised on the bottoms of her feet ... the bruising and blisters on the soles of her feet were
caused by staff allowing her feet to drag along the floor as they pushed her
wheelchair, rather than supporting them on the footrests.
· Made to suffer the indignity and trauma of being hoisted naked in a mechanical lift up under
the cold air vents in the ceiling; When we walked in and found her in this awful
state, staff said they were cleaning her and told us to leave.
· Found by hospital staff to be suffering a pressure sore at the base of her spine; to
our knowledge no wound care was previously given by the nursing home
· Deprived of the right at our request - to be moved to a more compassionate competent
care setting
When our loved one died, we told her story to the CEO of the Regional Health Authority and
showed our photographs of the unconscionable harm caused to her. The CEO agreed our
loved one suffered an intolerable experience and promised to check into the situation and report
back to us. The CEO failed to keep his promise nothing was done. Our experience suggests
there is no accountability in this system that there is no will among the powers-that-be to take
responsible parties to task that elderly people like our loved one can suffer miserably at the
hands of health care professionals and no one of authority cares enough to right the wrongs.
The question we ask this government is: "What are you prepared to do to stop the needless
harm and suffering in our nursing homes?"
16
A Son's Testimony
My experience with my mother, so far has been fairly positive. On the other hand, I
have observed several incidences where a resident has been allowed to stay long in
wet incontinent wear. Also individuals are not properly washed and then develop a rash
and other times worse complications like urinary tract infection. Sometimes medication
is not administered properly because staff is switched and they are inadequately
instructed and with no clear direction they become frustrated and inattentive to a sense
of urgency and following procedures. In cases where oxygen is required, the resident
often will be without oxygen for hours due to lack of adequate staff or sense of urgency
and necessity. The ultimate question for government officials, nursing home owners and
workers is, "If it were you, right now, would you appreciate this kind of care?"
The resignation on the part of the family is ' what can we do about it?' I feel that
adequate standards are missing or not implemented consistently as deriguer.
My question to this government is: Are you committed to help the elderly in nursing
homes have a quality of life they deserve and have a right to?
Sincerely,
Rocco Angelozzi
17
A Daughter's Testimony
Two words that sum up me experiences with Long Term Care Facilities in the past six (6) years
are UNSATISFACTORY AND SCAREY.
1) OVERWORKED STAFF
Nursing Aides had 70 residents to care for with 4 or 5 staff on evening shift. Half of these
residents were wheelchair reliant, perhaps 8-10 were complete bed care with feeding etc., 10
relied on a walker and the remainder were mobile. If it was flu season or someone returned
from hospital, the number of caregivers did not change.
2) MINIMAL TRAINING REQUIREMENT FOR CARE WORKERS
Some new staff would ask my mother (97 yrs) how to operate the mechanical lift. One staff
member dropped her in the bath tub by neglecting to place her seat belt on when she was on
the tub lift. There are too many falls that take up too much Emergency Room time to say
nothing of the stress to the residents. My mother fell and spent 24 hours in the ER and
another 7 days on a busy Surgery Unit to discover that the fracture in her hip was an old
one!!!!!! Isn't that a surprise. Many many letters were written at that time with very pat
answers.
3) VALUE OF OUR ELDERLY STANDARDS AND ABUSE
There is a very thin line between abuse and poor care. One young hard working caregiver
told me about her first day on the job at another facility in Calgary. She did not return after
day 1 because of the poor treatment of the elderly there by the staff. She did not complain to
management because according too many of these workers, "it falls on deaf ears."
The 2 latest studies on the Healthcare System have echoed my sentiments. They totally ignored
the elderly in our Long Term Care System.
18
A Daughter's Testimony
My Mother is an 88 year old stroke victim who has been in nursing home care
and unable to walk since 1997. Many disturbing occurrences in her life have us
questioning the 'Alberta Advantage', however this one was life threatening.
On April 18, 2002, the day before Mom's 88th birthday, a telephone call
about 8:30 in the morning alerted me to the fact that an accident had happened to
my Mother. My Mother had suffered two falls recently (March 20 and April 1)
therefore I rushed to her residence to see for myself what had happened. I
arrived within 10 minutes of the call and made sure, this time, to take a camera
with me. As the photos show, Mom was laying on the floor, her head being
stabilized by a staff person. Mom lay on the floor until 10:30 when paramedics
arrived to transport her to emergency for treatment.
To date, no administrative explanation or apology has been given to our family.
HOWEVER -- Attendant and care-giving staff (including the senior care-giver at
the occurrence) have told me that Mom was in the sole care of an inexperienced
new staff person. This person, by herself, was attempting to move my Mother in
the lift while the senior staff person was attending to the needs of another
resident. My Mother slid out of the lift and fell fully backwards with such force
that her head required staples to close the bleeding wound.
My Mother's safety was placed at risk because of this decision and this action.
Further --
My Mother suffered a severe concussion that has left her more noticeably
confused and frustrated. She becomes extremely emotional and weepy. She has a
difficult time trusting any caregiver unless she sees them and can relate to them
consistently. She reacts with extreme fear whenever she sees a lift, and we have
instructed staff that a lift should not be used with her. She lost about 20 pounds
(she now weighs about 115 pounds) in a very short time, and we discovered that she
could not even feed herself because of weakness - thus necessitating hiring of
feeders when family cannot attend to ensure that adequate nutrition is a daily
guarantee.
19
A Wife's Testimony
EVENTS CONCERNING MY HUSBAND'S CARE
In care since January, 2001
(1) Dehydration.
(2) Gland infection due to lack of oral hygiene.
These two problems led to 3 weeks hospitalization with several days when he was
semi-conscious.
(3) Physical attack . Injuries to face. Refusal of senior staff to report this to
PPIC. I reported the incident and an investigator was appointed to the case.
Photographs were taken as evidence, although the investigator would not take a
copy of the photos with her. The final report from PPIC stated that there was a
lack of evidence.
(4) Physiotherapist cancelled walking program over 1 year ago. After 14 months
he is still walking with me, assisted by the Director of Care at the facility.
(5) After allegations of his being aggressive I was requested to give permission
for him to be given Risperdal, an anti-psychotic drug. I disagreed, and said that I
would not agree to any medication being given until the RN investigated the reason
for the so called "aggression". This was done, and malfunctioning equipment was
found to be the main cause of the problem. Arrangements were made for this
equipment to be avoided. Staff had no further wish to administer Risperdal.
More staff would obviously eliminate some of the problems, but also
determination by senior staff to investigate and resolve difficulties before using
drugs could bring a quicker and better result.
There are so many residents who have no one to speak for them, so I feel it is also
essential that there should be inspections carried out at facilities, without previous
notice being given.
20
A Daughter's Testimony - Tina's Story
In August 1995, my mother was placed into a long-term care facility. They immediately
changed all her medications, and began to administer Prozac to calm her. In January
1996 she suffered a bleeding ulcer and was found on the floor. The blood loss and
transfusion caused a stroke that paralyzed her.
Her health & quality of life after the stroke deteriorated - any concerns that I voiced were
dismissed or ignored. She received more medications and less care. A senior nurse
once told me that these old fogies are only here waiting to die anyway.
Mom was near death and rushed into the hospital two more times over 2 years, the last
time in a diabetic coma with blood sugar levels over 80 and infected bed sores.
What gives the right to these care facilities to drug their residents needlessly? I was
often told it was because they were understaffed and the drugging made it easier for the
staff. Our health care system pays for the unnecessary, over-medication of seniors in
care facilities when this money could go toward hiring quality staff and better policing of
these facilities to ensure the proper care of the residents. Where is the care, respect
and dignity our elderly deserve have they not earned it?
Thank you.
21
A Daughter's Testimony
My Father Arnold Kauppila passed away Nov 9th 2001. I, with the help
of my husband and daughters, looked after my father for the last ten
years. My father had Alzheimer's. In the last ten years my experiences
with hospitals and nursing homes have been horrifying. The first nursing
home was Glenmore where my father packed his bags and paid some
guy on the street $5.00 to drive him from Glenmore Trail to Forest
Lawn. Thank God he wasn't found in a ditch somewhere. Over an hour
later when the nursing home was contacted, we were told he was down
the hall playing cards. They had no idea he was gone! He packed his
suitcases and left. Some years later, I mistakenly entrusted the care of
my father to the system again at Forest Grove where I got three phone
calls a day. They had no idea of how to work with an Alzheimer's
patient. They withheld vital pain medication which, to me, was cruel,
and tried to chemically restrain him with Risperdal. Medication was not
written down and blood tests weren't given when they were supposed to.
I constantly had to argue with Forest Grove. It was more stressful and
dangerous to have him in this nursing home than to have him at home.
After thirty days and a hospital stay, I brought him back home. I am still
arguing with Forest Grove because they are trying to over- charge us.
Seniors have built this country and deserve to be looked after and safe.
It's our obligation to make this happen. If it was not for them, Canada
would not be what it is today and we owe it to them. Someday we may
be seniors too.
Sherry Lester
22
A Daughter's Testimony
ABUSE OF MY ELDERLY MOTHER
My Mother was a resident in a Calgary nursing home. In one year she had sixteen
falls resulting in cuts, bruises, a possible broken rib and, on one occasion, was too
hurt to walk. She was never x-rayed, and a doctor examined her for these injuries
only twice.
Mom told us that she had been beaten by a staff member. Her nurse was later fired
after being observed knocking an elderly resident to the floor. I saw a nurse grab
Mom's face and yell at her.
When Mom developed raw, painful sores on her back and my requests for a
physician assessment were ignored, I took her to a dermatologist who diagnosed an
untreated staph infection.
On another occasion, a rapid decline in Mom's health was minimized by nursing
staff as the flu, when in fact she was suffering life-threatening dehydration due to a
lack of fluids, as diagnosed by her physician.
She sometimes was not fed, and she was often soaked in urine.
Mom passed away from pneumonia after her blatant symptoms of lung congestion
and depleted oxygen levels were deemed by nurses to be only the sniffles. When I
challenged their observations, I was admonished for being over-protective.
I have concluded that despite my heroic efforts, I could not protect my Mother
from the inadequacies of this facility.
23
A Daughter-in-law's Testimony
Muriel Freeman (my mother-in-law) entered Mayfair Nursing Home at the end
of August 2001. She was moved to the Vulcan Nursing Home on November 26,
2001. Muriel passed away two months later on January 22, 2002 from
dehydration and pneumonia.
The four months in Mayfair, I witnessed:
· Over medication
· At times staff would not take Muriel to the bathroom when she asked.
· She become so weak and hunched over and left sitting in one position
for long periods.
· She became dehydrated.
· Toenails were uncut. They started to curl under.
· Staff used hoists and handled her roughly. They ignored her pain.
· They lost personal items.
· Muriel was given only one bath a week.
· Staff lifted her skirt and checked if she was wet in front of visitors.
It does not cost more to treat a human being with respect and
compassion. Homes need to be held accountable for their treatment of
our elderly.
24
A Daughter and Son-in-law's Testimony
After two years at our home Anna went to a nursing home. In the four years that she has been
there she has been hospitalized twice suffering from pneumonia, dehydration and lack of
nutrition. During her nursing home care she has had three fractures (pelvis (twice) and ribs).
We have witnessed people unable to feed themselves and not being helped, people without teeth
given regular food, drinks placed beyond the reach of the residents, full drinks replaced with new
drinks with no concern that the previous drinks were untouched. Plus we have seen and
experienced much, much more.
Our deepest wish is that these nearly helpless seniors would someday receive at least as much
concern and protection as children in a day care. In many ways they are the same as children but
lack the ability to complain and speak on their own behalf.
25
Testimony of The Hamel Family
The Experiences of Margaret Hamel, while a resident of the Bethany Care Centre, Calgary.
Mother of 12, Grandmother of 30.
My mom lived with a family member for three years after being diagnosed with Alzheimer's disease.
Then we placed Mom into a facility. I would love to say my mom was placed in a home, but Bethany
Care Calgary is a facility. We documented daily, not to find fault with the facility, but to keep our family
informed about changes in mom's condition and aspects of care. What we have now is a well-documented
journal of the facility. It starts with the staff and administrators. We need a Governing Accountable
Body. Nothing changes - incident reports are handed in and no results ever communicated to family
members; staff are transient, ill-trained and unmotivated to do more than what they MUST do ; staffing
ratio to patients are only sufficient when V.I.P.s are on their way. This facility would hire or allow more
hours when someone important was coming around. Did you know staff are given a quota of diapers
allowed to be used on a patient. 2 to 3 a day is the allotted amount?
Our critical overview of the facility
Suppertime Residents are herded to a dining area where they sit and wait up to an hour for dinner. Well
functioning patients are made to sit with residents that scream or do not want to sit at the table. Residents
are made to sit through meals with soiled diapers. Each resident is put in a bib, even if they are able to
feed themselves ( where is the dignity here).
Toileting. I had to get staff to help a resident who was walking the corridor with her depends to her
ankles... no one was paying attention. On several occasions we would come in to find my mom soaked
and embarrassed. When we addressed the obvious, the staff would blame the disease, " you know your
mom is progressing she will need diapers."
We purchased the store-bought variety of depends because they were better fitting than the ones provided
by the facility. We advised the nursing desk and the team leader that we had purchased them. It took over
two weeks for the staff to use them. We came in nearly every day to find my mom in her regular
undergarments soaked. No communication. When the diapers were incorporated into my mom's daily
attire, then no one would toilet her because she was in diapers. So then we come in and find her sitting in
soiled diapers.
Accountability - On more than one occasion that we know of my mom was given medication that was
not prescribed for her, but you could never find out why or who was responsible.
Once when we arrived to take Mom on a zoo outing, we were informed that she needed a suppository
because she hadn't had a bowel movement for x amount of days. When we phoned her daily private
caregiver to find out if this was true, she informed us that Mom is very regular and that she had informed
staff so they could chart it. However they didn't chart it, so the suppository would have resulted in
unnecessary physical discomfort and no outing. Apparently it is mandatory to keep track of such things,
however there is simply no point in rules that are not followed and no one is held accountable.
The restaurant business is inspected by random visits from health inspectors. If the establishment doesn't
meet code they are shut down for a day, a week, or until the requirements are met. The inspectors visit
unannounced, and sometimes at the busiest times of the day. We want to see unannounced visits to all
facilities at least yearly. We want satisfaction surveys sent to the guardians not the Alzheimer's patients.
( this actually happened ). We want the inspectors to have the authority to make demands for changes and
revisit to see that changes have been made. Residents are a lot more vulnerable than the average person
eating a meal in a restaurant. Maybe if a facility was closed down for a day and the residents had to be
moved, or the facility's subsidy was based on some aspect of these inspections and surveys - someone
might listen. I think the media would listen.
26
A Daughter's Testimony
My name is Angie Murray. I had a Father who lived in a care
centre 8 ½ years. This dear man was placed into the nursing home
with severe depression and a thyroid problem.
Unknowing to the family, he was put on Haldol, an antipsychotic.
He was on this drug for 6 ½ years. There was no documentation in
the clinical records concerning any significant side effects
from this medication. It was family that witnessed severe
drowsiness, drooling and hand tremors for over three years and
discussed their concerns to staff.
It was I that demanded he be taken off this drug after I was put
wise that something was going on here. He suffered terrible
adverse side affects, including involuntary muscle movements,
tongue darting, rocking and difficulty speaking. These side
affects are irreversible.
We feel this is a criminal offence. It's no different than a
drug-pusher in a schoolground pushing drugs destroying young
lives. The same applies in the nursing homes. What gives them
the power to destroy the elderly and tear the hearts out of
families?
27
A Daughter's Testimony
My name is Beverley Mann. My mother lived in a nursing home for approximately four years,
during which time 1 was a constant visitor as 1 had many concerns with regards to the physical
and emotional care given to my mother.
This is one example: visit October 13, 2001
Failure of staff to follow doctor's order of offering a food supplement, the staff didn't know
where the supplement was kept. My mother would have gone to bed hungry had I not been
there.
Failure of staff to safely handle a one -person transfer resulting in my mother becoming
frightened and agitated and at risk of falling.
Failure of staff to provide needed skin care even though I mentioned to staff that my mother
had a rash on her bottom.
Failure of staff to provide a thorough evening wash, including pericare.
Administration's solution to the problem: To move staff member to another resident, or I could
move my mother to another facility.
Final Comment: My mother died in the hospital on October 31, 2001 with a scalding rash to her
bottom and groin --- an indication of no improvement since October 13th.
I've come to the conclusion that I hope not to live long enough to endure life in a nursing home.
28
A Daughter's Testimony
My mother is 98 years old and has been a resident in a nursing
home in Lacombe for the past 8 years. She spends all day in her
wheelchair, and over the years with the budget cuts we have seen a
deterioration in the care the staff give her. Family members have seen
her not warmly wrapped, with her knees covered with an afghan and
the back of her legs bare and cold. A lot of the time the staff neglect to
place her call bell where she can reach it, and many a time she has not a
supply of water where she can reach it (and this in the middle of July)
Mom is one of the few residents who reads, yet they do not always
have her curtains pulled and the reading lights on. Many a time they
wheel her in and leave her in the middle of the room where she cannot
reach anything. My sister and I who visit the most regularly have
spoken to the staff time and time again about her neglected care. Once
in awhile we will visit and find all things done as they should be. But
why do family members always have to harp about her care?
To our government officials, I say, you may be a resident some day in a
nursing home. See what you have to look forward to.
Marion Wooden, Calgary
29
A Son's Testimony
The care of our seniors today is a serious problem due to the fact that
the institutions that care for them are very understaffed and have very little
training in eldercare.
To look after children in daycare, you must have proper training and
adequate staff. When it comes to the elderly, it almost seems the attitude
is: Who cares, these people are at the end of the life and are no longer
productive, so why waste time and money on them? Why do the elderly
have to be treated like the leftovers of society?
I think government has a responsibility to ensure that seniors' rights
and living conditions are protected.
Funding is an issue that has been talked about a lot. The homes that
care for the elderly always say that there is not enough funding. Let's have
the homes tell the public where the money spent. Make them accountable
for the funds they receive from the governments and the funds paid by the
seniors.
Financial statements are public knowledge. Approximately $4000.00
per person is paid to homes from the governments and the person residing
there. I believe there is a lot of money that is not accounted for after the
homes or institutions receive it.
The home my parent is in has 80 residents. That means the
institution receives about $320,000.00 a month which works out to about
$3,840,000.00 a year. You would think that a sum of money such as that
would ensure proper care, but as we've seen time and time again, it has
not.
There needs to be a better accountable system that utilizes the funds
for proper training, better meals, proper equipment and overall better care
of our elderly.
Murray Carson
30
A Sister-in-law's Testimony
Hospital Care
My name is Linda Iverson. On May 23, 2002, my brother-in-law, Fred Iverson
was released from the Peter Lougheed Centre. Before I got him out the front door,
he coded. I took him around to the E.R. where they worked on him to get him
stabilized. But they would not readmit him. The "Doctor" said to take him home.
He said how I got him there was not his problem. Fred was taken by ambulance to
the Crossbow Transition Unit where the head nurse told me that he was much too
sick to be released. Fred was in the Crossbow for seven days. While he was there,
his oxygen tubes came undone twice. They said that he disconnected them
himself. My husband could not pull these tubes apart, so how could a man as weak
as Fred pull them apart? In conclusion, it is my opinion that the Alberta Medicare
System does not care if you live or die, as long as you don't die on their premises.
31
A Family Testimony
The base of our concerns as experienced with our parent is as follows:
- inadequate care
- not enough care givers
- many staff, if not most, are not trained in the disease they are administering to
- staff morale is very low
- unrealistic job descriptions
- no obvious valuing of these jobs by administration and/or society
- cuts in middle management have created unrealistic job duties which cannot be performed properly
- staff has been intimidated into negative advocating role that encourages no voicing of problems for
fear of personal disciplinary repercussion and/or further funding cuts
- not enough supplies and equipment to allow for safety of patients, cleanliness to ensure healthy
environment or basic needs which guarantee a degree of comfort and dignity
Most, if not all, of this can be blamed on inadequate amount of money being given and directed towards
the frontline problem areas, such as more care givers and proper training.
Our parent homesteaded literally to help build this province. She spent a lifetime raising a family that has
contributed to and been proud of Alberta and Canada. It is shocking that we spend more per day on a
prisoner in a jail, than on our elders in our care facilities. Maybe it is time for some militant action to be
taken in the form of a civil suit against the government, in order to protect our parents, and make old age
decent for our generation and for you and your family.
32
CONCERNS OF FAMILIES WITH LOVED ONES IN RIVERCREST NURSING HOME
RESIDENT CARE
NUTRITION /HYDRATION ... continued
1. Weekly baths not adequate
4. Inconsistent assistance for those who can't
2. Pericare not sufficient (Use rolled-up wet
manage to drink on their own
toilet paper for personal cleanup)
5. If fluids are spilled by a resident, not
3. Residents sometimes smell of urine and
reoffered or replaced
feces
6. Poor quality of food
4. Toileting routines not appropriate
7. Poorly balanced meals (e.g. no vegetables at
5. Residents encouraged to use incontinent
lunch)
supplies rather than toilet
8. Special diets not observed
6. Some residents left in soiled incontinent
9. Residents may not be able to eat the meal
supplies for too long (e.g. some wheelchair
(eg: not ground for residents with no teeth,
cushions are soaked with urine)
sandwiches for residents who have difficulty
7. Some residents wait on toilet for help for 45
swallowing)
minutes
10. Some residents refuse to eat due to poor
8. Bladder training every two hours is not
taste, poor presentation and meal
consistently observed by staff
unappetizing
9. Improve mouth care not all residents can
11. Food is too cold and coffee too hot
manage to brush their own teeth or to clean
12. Some residents have missed their meals if
dentures; frequently mouth care is not
they are not in the dining room
provided
13. Staff have been observed to finger feed two
10. Staff do not clean residents appropriately
residents simultaneously/or use same
after meals (e.g. soiled clothing)
utensils for both'
14. Poor hand-washing technique in the kitchen
RESIDENT COMFORT, SAFETY,
(staff smoke outside and do not wash hands
MOBILIZATION
upon return)
1. Some residents wait for call bell to be
15. Dietician not responsive to expressions of
answered for 1 hour +
concern
2. Inadequate help for residents to dress
appropriately and comfortably (e.g. the right
STAFFING AND RELATED ISSUES
shoes, hair care)
1. Families feel inadequate staff (Re: Ratio to
3. Family felt staff did not notify them in a
residents not enough staff to feed, toilet,
timely manner re incident of falling, resident
bath, mobilize)
missing, etc.
2. Staff require more training
4. Family felt some residents inappropriately
3. Proper transfers not being done:
put in wheelchairs and restrained and not
- do not use transfer belts appropriately
mobilized enough
- do not use 2 person transfer when
5. Gloves infrequently used by staff
necessary
6. Inadequate staff hand washing between
- not all staff appear to be appropriately
resident care
trained to feed
7. Rinsing of bed pans in sinks, subsequent
4. Some staff are rough and do nor give
sinks are not disinfected or properly cleaned
compassionate care (eg. When moving
prior to resident use
residents)
8. Care plans are posted but not consistently
5. Good staff who are competent are stretched
adhered to or changed in accordance with
"too thin" and "run ragged"
resident's changing needs
6. Some families hire private individuals to
feed their family member
NUTRITION /HYDRATION
7. Some families do nor feel confident in
1. Inadequate hydration is a major problem
staff's ability to manage residents' care
2. Poor hydration of residents has sometimes
when family members are away (e.g.
resulted in the need for residents to attend
vacations, business trips, etc.) and, in fact,
hospital
would not go away on vacation without
3. not all residents receive fluids or snacks (eg
hiring someone to assist with resident's care
diabetics) on a consistent basis
33
STAFFING AND RELATED ISSUES .. cont'd
PERCEPTIONS OF STAFF ... continued
8. Families are expected to provide an
6. Feel management does not support/listen to
increasing amount of care for residents
staff concerns (Re workplace issues)
9. Staff take inappropriate breaks during busy
7. Lack of communication between shifts
times (eg. Before and after meal times,
8. High turnover of staff
during actual lunch and supper hours, staff
9. Too many good staff have left
sometimes go offsite for meals or to pick up
food)
ORGANIZATION OF LAUNDRY
10. Some staff not trained to give medications
1. Clothing frequently missing even when
properly
labeled
- on occasion medication mistakes
2. Nor sorted/delivered appropriately; residents
corrected by residents
frequently have on each other's clothing
- medications suspended and changed??
Doctors orders??
ADMINISTRATION
- Medications removed from floor if
1. Families do not feel local management
dropped and given to residents
listens/respects concerns
11. Families feel inadequate supervision re
2. Families fear repercussions to residents if
restraints in wheelchairs and residents who
concerns are voiced
have mobility problems; residents
(eg. Increase of personal injury to resident,;
wandering outside facility
threats of transfer or eviction)
12. Lack of walking program or appropriate
3. Some families feel local management is
exercise program
dictating direction of client care to the
13. Lack of supervision to ensure client care is
detriment of residents and family support
adequate
14. Families' request for crushed/liquid meds
MATERIALS MANAGEMENT
not met
1. No dishwasher dishes done by hand
15. Staff take extended breaks in evenings in
2. Insulated cups are old and are not sanitary
meeting room with lights out when
3. Plastic water glasses washed and reused
management not around
4. Plastic medication cups washed and reused
16. Recreation staff and activities not adequate
5. No straws available
17. Staff socializing with each other during
6. No spill-proof cups for residents who
residents' meal rather than with residents
require them
18. Staff do not appear to be diligent about the
7. Mattresses not replaced appropriately;
care of residents' belongings
families told to buy foam mattresses
(eg. Hearing aides, glasses, clothing,
8. Inadequate/archaic physio equipment
dentures, and staff not particularly helpful in
finding lost items)
BUILDING MAINTENANCE
19. Family feel inappropriate medication used
1. Smoking area is not contained or vented
for control of resident behaviour and also
2. Smoke filters through hallways and
disagree with staff perception of what
throughout facility
constitutes aggressive tendencies
3. Air quality is poor
20. Some families feel physician visits and
4. Poor ventilation in summer; no air
coverage not acceptable
conditioning in common areas
5. Exhaust fans in hallway not working
THE FOLLOWING PERCEPTIONS OF
STAFF WITHIN THE FACILITY WERE
EXPRESSED
1. Lack of supervision and leadership
2. Poor morale generally
3. Plotting, back stabbing
4. Insecure feel job repercussions if they
voice concerns
5. Inadequate training and educational
opportunities
34
35
Appendix A
Following is a small sample of FAIRE's efforts to advise the Alberta government of residents'
experiences of abuse, neglect and poor care, and the urgent need to address the root causes.
1. FAIRE's 1999 Report:
An Initiative Addressing The Needs and Rights of Alberta's Nursing Home Residents
This report draws attention to Alberta's appallingly lax Nursing Homes Act and Regulations through a
comparison of regulatory standards and legislated residents' rights from other jurisdictions, including
Ontario, British Columbia and New South Wales. FAIRE called on Alberta Health and 3 MLAs to use the
content of this report as a framework for reforming Alberta's Nursing Home legislation. There was no
response.
2. FAIRE's January 2000 letter to the Premier
This letter called for a meeting to discuss the growing reports of residents' experiences of abuse and
neglect, and an action plan to address the contributing factors. The Minister of Health responded in
the Premier's stead, saying the Premier's schedule did not allow for him to meet with us.
3. FAIRE's October 2000 Meeting with the Associate Minister of Health
This meeting drew awareness to systemic flaws that are endangering the health, safety and lives of
nursing home residents. FAIRE called on the Minister to respond to our recommendations that included:
I) the development of effective legislative safeguards for nursing home residents; 2) increased numbers
of skilled front-line staff 3) the development of policies and standards for strengthening the mandate of
the Health Facilities Review Committee. There was no response.
4. FAIRE's October 2000 Meeting with the Calgary Conservative Caucus
This meeting involved two family members who used personal photographs to relate their loved ones'
experiences of nursing home abuse and neglect. FAIRE presented a summary of regulatory deficiencies
that contribute to the problem, and called on Caucus to work with the Associate Minister to address these
longstanding flaws. There was no response.
5. FAIRE's September 2001 Report: The Shame of Canada's Nursing Homes
This research-based report examines abuse and neglect of nursing home residents from a national
perspective. Distribution of the report included Premiers and Ministers of Health of the Provinces and
Territories. There was no response from Alberta's Premier. The Minister of Health & Wellness sent
a letter of appreciation.
6. FAIRE's March 2002 Letter to the Minister of Health & Wellness
This letter provides a detailed account of deficiencies plaguing Alberta's long-term care system and the
serious ramifications for residents. FAIRE's recommendations focused on 4 key contributing factors: 1)
lax regulatory standards 2) chronic underfunding 3) lax inspections and enforcement of standards 4)
lack of sanctions. The Minister's response showed no discernible understanding of the seriousness
of the problem or the urgent need for immediate remedial action.
7. FAIRE's May 2002 Forum: Speaking Out Against Abuse and Neglect in Our Nursing Homes
FAIRE's report, The Shame of Canada's Nursing Homes, was launched at this public awareness event
which drew more than 125 people. Our guest speaker was Charmaine Spencer, lawyer and researcher of
vulnerable populations at Simon Fraser University. Invitations were sent to the Premier, every Minister
and MLA. None attended.
36
Appendix B ... Current Minimum Staffing Standards in Alberta
Under Sections 14(5)(6) of Alberta's Nursing Homes Operation Regulation, an operator is
required to provide an average of at least 1.90 paid hours of combined nursing and personal
services to each resident per day with at least 22% of combined services provided by nurses.
These non-specific minimum standards translate into dangerously-low staffing levels as
reflected in the following information provided by Extendicare administration at the request of a
family member.
EXTENDICARE CEDARS VILLA
STAFFING PATTERNS as of August 10, 1998
Unit
Census
Days
Eves
Nights
Primrose 35
1RN
1RN/LPN
1/3RN
2PCA
1.9PCA
1PCA
Willow
33
1RN
1RN
1/3RN
2PCA
1.9
PCA 1PCA
Larkspur 47
1RN
1RN
1/3RN
3.7PCA
3.3PCA
2PCA
Clover
54
1RN
1RN
1/3RN
1LPN
.4LPN
2PCA
4PCA
3.3 PCA
Maple
40
1RN
1RN
1/3RN
1LPN
3PCA
1PCA
3.7PCA
3PCA
Poplar
39
1RN
1RN
1/3RN
1LPN
3PCA
2PCA
3.7PCA
Formula for Determining Compliance with the Required 22% RN Component
·
248 residents X 1.9 hours = 471 total care hours per day
·
22% of 471 total hours = 103.6 required hours of RN care = 0.42 hr care per resident per day divided by 3
shifts = approx. 14 minutes of RN care per resident per shift
·
103.6 RN hours divided by 7.5 hour shifts = 13.8 RNs in a 24 hr. period
·
Extendicare has 14 RNs indicating the facility is complying with Section 14(6) of the Nursing Homes Act.
Average Staff-to-Resident Ratios:
Days:
1 RN for 41 residents
(248 divided by 6 RNs)
1 LPN/PCA for 11 residents
(248 divided by 22.7 LPN/PCA staff)
Evenings: 1 RN/LPN for 39 residents
(248 divided by 6.4 RNs/LPNs)
I PCA for 12 residents
(248 divided by 19.4 PCAs)
Nights:
1 RN for 124 residents
(248 divided by 2 RNs)
1 PCA for 28 residents
(248 divided by 9 PCAs)
37
Appendix C
Following are recommendations from a research paper developed by a panel of experts in
response to the need for improved staffing standards to accommodate the increased acuity of
residents in nursing homes in the United States. These recommended standards specify the
amount and type of nursing staff and education /training levels considered as essential to meet
minimum daily standard. As shown in Appendix B, Alberta's staffing levels fall well below
these recommended minimum standards.
Administration Standard
· Full-time RN with a bachelor's degree as director of nursing ( a provision for grandfathering current RN directors
would be allowed for a specified period)
· Part-time RN assistant director of nursing (full-time in facilities of 100 beds or more; this person may also be the
MDS coordinator)
· Part-time RN director of in-service education ( preferably with gerontology training; full-time in facilities of 100 or
more)
· Full-time RN nursing facility supervisor on duty at all times, 24 hr/day, 7days/week
Direct Care Staffing Standard
The minimum number of direct care staff must be distributed as follows:
Minimum level direct care staff (RN, LVN/LPN or CNA)
Day shift
1FTE for each 5 residents
(1.60 hr per resident day)
Evening shift
1FTE for each 10 residents
(0.80 hr per residents day)
Night shift
1FTE for each 15 residents
(0.53 hr per resident day)
Minimum licensed nurses (RN and LVN/LPN) providing direct care, treatment and medications, planning,
coordination, and supervision at the unit level:
Day shift
1FTE for each 15 residents
(0.53 hr per resident day)
Evening shift
1FTE for each 20 residents
(0.40 hr per resident day)
Night shift
1FTE for each 30 residents
(0.27 hr per resident day)
Minimum total number of direct nursing staff is 4.13 hr per resident day. Total administrative and direct and
indirect nursing hours is 4.55 hr per resident day. Staffing must be ADJUSTED UPWARD for residents with higher
nursing care needs.
Mealtime Nursing Staff
Direct care staff standards will take into account specific needs of residents at mealtimes. At all
mealtimes there will be:
· 1 nursing FTE for each 2-3 residents who are entirely dependent on assistance
· 1 nursing FTE for each 2-4 residents who are partially dependent on assistance
Nursing staff who assist with feeding should be CNAs who are adequately trained in feeding procedures and they
should be supervised by licensed nurses.
Education and Training
All licensed nurses in nursing homes must have continuing education in care of the chronically ill and disabled and/or
gerontological nursing (at least 30 hr every 2 years)
NAs should have a minimum of 160 hr of training, including training in appropriate feeding techniques.
Nurse Practitioners
Each nursing home is strongly urged (but not required) to have a part-time geriatric or adult nurse practitioner and/or
a geriatric clinical nurse specialist on staff (full-time for 100 beds or more).
Note:
RN = registered nurse; MDS = minimum data set; LVN/LPN = licensed vocational nurse/licensed practical
nurse; CNA = certified nurse assistant; FTE = full-time employee; NA= nursing assistant
Builds on the Nurse Staffing Standards accepted by the National Citizen's Coalition for Nursing Home Reform (1995).
Resource: Experts Recommend Minimum Nurse Staffing Standards for Nursing Facilities
Harrington C. PhD,RN, FAAN - Kover C. PHD,RN,FAAN - Mezey M. PhD, RN, FAAN - Kayser-Jones J. PhD, RN,
FAAN - Burger S. RN, MPH - Mohler M. RN, MN, MHSA - Burke R. PhD - Zimmerman D. PhD
38

Appendix D
An autonomous family
A family council usually has a staff advisor
council is an organized, self-
who supports and assists the council, but
led, self-determining,
is not considered a council member.
democratic, consumer group
However, councils are free to operate
composed of families and
without a staff advisor if they choose.
friends of residents living in
long-term care facilities.
The emphasis of all family councils
is mutual support, empowerment
A family council has two
and advocacy.
main goals:
· To protect and improve
the quality of life of
residents
Each council will be unique. There are no
hard and fast rules about how a council
· To give families a voice
should organize or operate, or how it
in actions and decisions
should meet the needs of its members,
that affect them and the
residents and the facility.
residents of the facility
Common to all family councils is the commitment to provide families a forum in
which to openly express their concerns and ideas, and a way work together for
positive change.
Produced by Families Allied to Influence Responsible Eldercare (FAIRE)
39